The upper limb surgery (therefore, shoulder surgery) and the corresponding rehabilitation treatment influence greatly the final outcome.
Although every procedure is different, they share similar characteristics.
The movilisation must be early in the treatment. In the first place the joint movilisation will be passive, and motion degree will increase progressively.
Therapy should not be painful, specially during the first weeks which are usually focused on recovering motion and lessening the pain.
From 4 weeks on, it is recommended that the beginning of movilisation should be active and against resistance. This sort of rehabilitation must be controlled by a physiotherapist all the time. Going to the swimming pool can be a very good choice to make progress in the water.
Fusce risus mauris, consequat nec suscipit quis, hendrerit eu sem. Aliquam sed ipsum dolor. Sed molestie lacinia felis in iaculis. Curabitur congue luctus purus, vitae pretium purus aliquet eu. Etiam elit metus, luctus eget scelerisque vel, rutrum in lorem. Fusce nibh magna, condimentum faucibus consectetur sit amet, facilisis id eros. Duis quis sodales elit. In vel porttitor augue. Mauris et turpis ante.
PREOPERATIVE STEP
In the consulting room you will be given all the information about your pathology and the procedure to follow. Do not hesitate to ask anything that crosses your mind.
We will provide you an e-mail address where you can solve any doubts and any other questions you may have in hindsight.
You will be also given the informed consent as part of the process.
The day of the intervention you should be hospitalized 2-3hours before, the time we need for your pre-surgical preparation (we will insert an intravenous line into one of your arms, supply pre-surgery medication, etc.)
Remember to fast, it means that you should not eat or drink anything for 8 hours before the surgical procedure.
INTRAOPERATIVE STEP
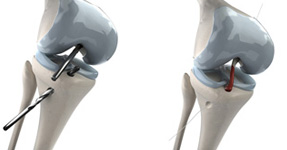
Shoulder arthroscopy is a minimal invasive technique. It entails the insertion of specialized optical and surgical instruments into your shoulder joint by means of small incisions. Time in the operating room will not be long but it depends on the method undertaken. The shortest intervention is the acromioplasty, it may last 45 minutes. The longest one is the relapsing shoulder dislocation that may last even 120 minutes.
General anesthesia is commonly used, together with a locoregional technique that consists of a brachial plexus block aimed at controlling efficiently the pain during first postoperative hours.
The patient will wake up with an adequately immobilized shoulder.
POSTOPERATIVE STEP
Shoulder arthroscopy can be an outpatient procedure. The patient has two options after surgery: being hospitalized just one night or being discharged.
By the end of the operation the patient will be informed of the procedure performed and the findings during the course of the intervention.
Your surgeon will give you the discharge report, some recommendations and the treatment to be followed and future medical appointments in the outpatient consultation.
Postoperative management:
It may be possible that your shoulder hurts after the surgery and the following days. Swelling can also affect the area but the symptoms are controlled with the recommended medication shown in the discharge report.
You will use a sling for 2-4 weeks and be allowed to move the elbow, hand and fingers twice a day.
The removal of stitches will be done 10-15 days after the surgery, with the immediate start of the rehabilitation therapy.
After hospital discharge you should keep in touch with the surgeon if there is uncontrolable pain, fever, redness and wound drainage or any complications.
Joint surgical treatment revolution, which began in 1912, has considered Arthroscopy as one of the biggest contributions to the Orthopaedic Surgery of the twentieth century. The same has happened with arthroplasties.
The use of the arthroscope lets the surgeon carry out less aggressive surgical techniques, what have contributed to the open surgical techniques of the meniscus, cruciate ligament or tendinous injuries be replaced for these arthroscopic procedures.
")
")
")